
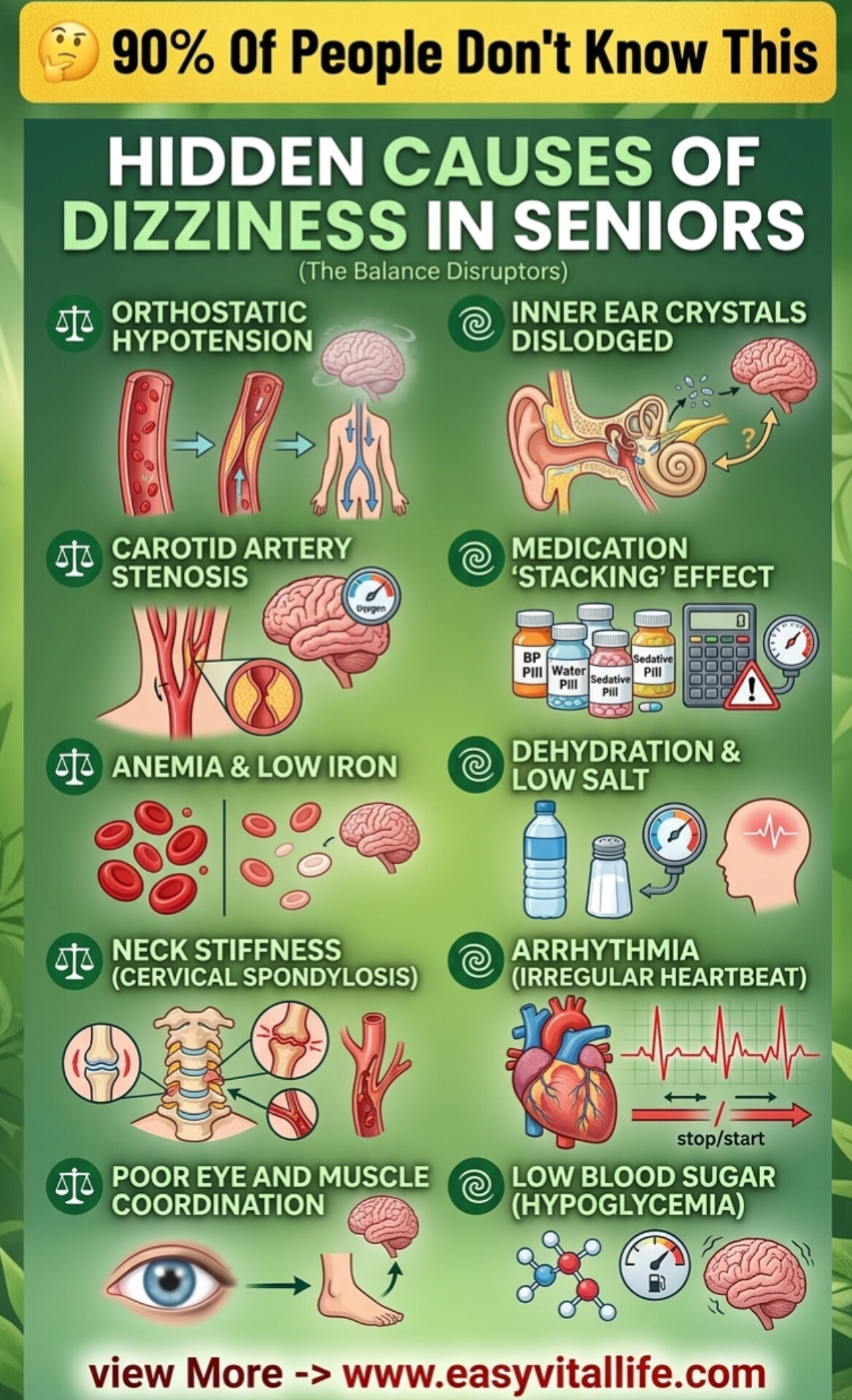
Hidden Causes of Dizziness in Seniors: Understanding the Balance Disruptors That 90% of People Don’t Know About
Dizziness affects more than fifty percent of people over age sixty-five, making it one of the most common health complaints in seniors. However, most people attribute dizziness to vague causes or accept it as an inevitable part of aging…
The truth is that dizziness typically results from specific, diagnosable medical conditions that are often overlooked during standard medical evaluations. Understanding these hidden causes of dizziness empowers you to identify the root problem and pursue targeted treatment rather than simply managing symptoms. This comprehensive guide explores ten major causes of dizziness in seniors and explains why conventional medical approaches often miss these critical underlying conditions.
Dizziness is not a disease itself but rather a symptom indicating something specific is wrong with your balance system, cardiovascular system, or neurological function. Your brain integrates information from your inner ear, eyes, muscles, and cardiovascular system to maintain balance and spatial awareness. When any of these systems malfunction, dizziness results. By identifying which system is malfunctioning, targeted treatment can restore balance and eliminate dizziness entirely.
Orthostatic Hypotension: The Pressure Drop When Standing
Orthostatic hypotension represents one of the most common and most overlooked causes of dizziness in seniors. This condition involves a sudden drop in blood pressure when standing from sitting or lying down. As blood pressure drops, the brain receives less oxygen, causing dizziness, lightheadedness, and sometimes fainting.
The mechanism involves the autonomic nervous system, which automatically adjusts blood pressure when you change positions. In seniors, this reflex often becomes sluggish, failing to increase blood pressure quickly enough when standing. The blood vessels don’t constrict properly, blood pools in the legs due to gravity, and brain blood flow drops momentarily.
Multiple factors contribute to orthostatic hypotension including dehydration, which is endemic in seniors who don’t drink enough water. Medications like blood pressure drugs, diuretics, and certain antidepressants exacerbate the problem. Prolonged bed rest, inactivity, and muscle weakness reduce the body’s ability to pump blood against gravity. Iron deficiency and anemia further impair oxygen-carrying capacity.
Treatment involves addressing the underlying causes. Increasing water intake prevents dehydration. Adding salt to the diet supports blood volume and blood pressure stability, contrary to conventional advice that recommends salt restriction for all seniors. Compression stockings help pump blood from the legs. Standing slowly and allowing thirty seconds for blood pressure to stabilize prevents dizziness. Regular exercise strengthens muscles and improves cardiovascular reflexes.
Inner Ear Crystals Dislodged: BPPV and Balance Disruption
Benign Paroxysmal Positional Vertigo, or BPPV, results from calcium carbonate crystals in the inner ear becoming dislodged and floating in the fluid-filled semicircular canals. These crystals normally anchor themselves in a specific location, providing positional information to your brain about your head’s position in space. When dislodged, the crystals move through the fluid with head movements, sending confusing signals that create intense vertigo.
BPPV causes sudden episodes of severe spinning dizziness triggered by specific head movements, particularly turning over in bed, looking up, or bending down. The dizziness is brief but intensely unpleasant, often lasting seconds to minutes. Many people fear they’re having a stroke, though BPPV is benign and self-limited.
The cause of crystal dislodgement includes head injuries, even minor ones from falling or bumping your head. Osteoporosis and calcium metabolism abnormalities may contribute. Prolonged bed rest can trigger crystal displacement. Certain viral infections affecting the inner ear can precipitate crystal dislodgement.
The Dix-Hallpike maneuver can reposition dislodged crystals, providing immediate relief. This specific head movement performed by a healthcare provider allows gravity to return crystals to their proper location. Epley maneuver is another repositioning technique effective for crystal displacement. Most cases resolve within one to four weeks, though repositioning maneuvers can accelerate recovery.
Carotid Artery Stenosis: Reduced Brain Blood Flow
Carotid artery stenosis involves narrowing of the carotid arteries that supply blood to the brain. As plaque accumulates on arterial walls, the vessel diameter narrows, reducing blood flow to the brain. While severe stenosis risks stroke, moderate stenosis causes chronic dizziness and lightheadedness from insufficient brain blood flow.
Dizziness from carotid stenosis worsens with exertion, when brain oxygen demand increases but narrowed vessels cannot increase blood flow proportionally. Lightheadedness, difficulty concentrating, and mental fog accompany the dizziness. Some people experience visual disturbances or weakness.
Plaque formation results from decades of cholesterol accumulation, inflammation, and endothelial damage. High blood pressure, high cholesterol, smoking, and diabetes accelerate carotid stenosis development. Age and family history contribute to disease risk.
Diagnosis requires carotid ultrasound or advanced imaging. Treatment depends on stenosis severity. Mild to moderate stenosis responds to aggressive risk factor modification including blood pressure control, cholesterol management, smoking cessation, and aspirin therapy. Severe stenosis may require carotid endarterectomy, a surgical procedure removing plaque from the artery.
Medication Stacking Effect: Drug Interactions Causing Dizziness
Polypharmacy, or taking multiple medications simultaneously, creates complex drug interactions that seniors rarely understand. Medications often prescribed together can interact in ways that cause dizziness, despite each drug individually being appropriate.
Blood pressure medications lower blood pressure to prevent hypertension complications, but when combined, they may lower blood pressure excessively. Sedating medications accumulate when multiple sedating drugs are combined. Medications affecting the inner ear balance system can combine synergistically to cause severe dizziness. Anti-nausea medications, antihistamines, antidepressants, pain medications, and blood pressure drugs all affect balance through different mechanisms.
The “stacking effect” occurs when multiple medications affecting similar systems are combined, creating effects far exceeding any single drug’s effects. A senior taking a blood pressure medication plus a diuretic plus a diabetes medication affecting fluid balance may experience profound dizziness from the cumulative effect.
Solution requires comprehensive medication review. Many seniors benefit from deprescribing, which means systematically discontinuing unnecessary or redundant medications under medical supervision. Healthcare providers should specifically evaluate whether each medication remains necessary and whether dosages could be reduced. Often, simplifying the medication regimen dramatically improves dizziness.
Anemia and Low Iron: Oxygen Delivery Compromise
Anemia results from insufficient red blood cells or inadequate hemoglobin to carry oxygen throughout the body. Iron deficiency is the most common cause of anemia, affecting approximately thirty percent of older women. Without adequate iron, the body cannot produce enough healthy red blood cells to deliver oxygen to tissues including the brain.
Brain oxygen deprivation causes dizziness, lightheadedness, mental fog, and difficulty concentrating. Anemic individuals tire easily with exertion because muscles and brain don’t receive adequate oxygen. The dizziness worsens with activity when oxygen demand increases but oxygen delivery remains inadequate.
Iron absorption declines with age due to reduced stomach acid and decreased intestinal function. Digestive disorders including celiac disease, inflammatory bowel disease, and gastric surgery impair iron absorption. Chronic blood loss from gastrointestinal ulcers, polyps, or bleeding causes iron depletion. Some medications reduce stomach acid, impairing iron absorption.
Treatment addresses the underlying cause of iron deficiency. Iron supplementation restores hemoglobin levels, typically requiring three to six months for complete restoration. Dietary iron sources including red meat, organ meats, beans, and leafy greens support iron repletion. Vitamin C enhances iron absorption, while calcium and coffee inhibit absorption timing.
Neck Stiffness and Cervical Spondylosis: Vertebral Artery Compression
Cervical spondylosis involves degenerative changes in the cervical spine, where vertebrae develop bone spurs and discs bulge, narrowing the spaces through which nerves and blood vessels pass. The vertebral arteries run through small channels in cervical vertebrae, delivering blood to the back of the brain including balance centers.
When cervical spondylosis causes vertebral artery compression, blood flow to balance centers decreases, triggering dizziness. Head movements that twist or rotate the neck may further compress the artery, worsening dizziness. Many people with cervical spondylosis develop positional dizziness specifically triggered by head turning or extreme neck rotation.
Neck stiffness, chronic neck pain, and restricted neck movement accompany vertebral compression. Some people experience arm pain or numbness from nerve compression. Progressive stenosis can cause serious neurological complications including myelopathy.
Physical therapy addresses cervical spondylosis through gentle neck mobilization, strengthening exercises, and postural correction. Avoiding extreme neck positions and sudden head movements prevents symptom exacerbation. Anti-inflammatory medications and muscle relaxants provide symptom relief. Severe cases may require surgical decompression.
Dehydration and Low Salt: Electrolyte Disruption
Seniors often become severely dehydrated without realizing it. As people age, thirst sensation diminishes, meaning the body’s natural drinking trigger becomes unreliable. Additionally, medications including diuretics and blood pressure drugs increase fluid loss. Cognitive decline, difficulty swallowing, and reduced mobility limit water access.
Dehydration reduces blood volume, lowering blood pressure and brain blood flow, causing dizziness. Electrolyte imbalances accompany dehydration, with sodium and potassium imbalances directly disrupting balance center function in the inner ear. The combination of dehydration and electrolyte imbalance creates severe dizziness.
Additionally, the conventional recommendation to restrict salt applies only to people with specific conditions. Most seniors benefit from adequate salt intake because salt supports blood volume, blood pressure stability, and electrolyte balance. Severely restricted salt intake contributes to dizziness.
Treatment requires deliberate hydration habits. Rather than relying on thirst, seniors should drink water throughout the day regardless of thirst sensation. Adding salt to food increases blood volume and supports blood pressure stability. Electrolyte replacement through foods or supplements restores mineral balance. Some seniors benefit from oral hydration solutions containing glucose and electrolytes, which enhance absorption compared to plain water.
Irregular Heartbeat: Arrhythmia and Brain Blood Flow
Atrial fibrillation and other cardiac arrhythmias interrupt the heart’s efficient pumping action, causing irregular blood flow to the brain. When the heart beats chaotically, blood flow becomes unpredictable, sometimes delivering inadequate blood to the brain.
Dizziness from arrhythmias often accompanies heart palpitations, where people feel their heart racing, fluttering, or beating irregularly. Some arrhythmias are asymptomatic, causing only dizziness without obvious heart symptoms. Fainting or near-fainting episodes may accompany dizziness from severe arrhythmias.
Risk factors include age, high blood pressure, heart disease, hyperthyroidism, and sleep apnea. Certain medications and stimulants including caffeine and ephedrine trigger arrhythmias.
Diagnosis requires cardiac monitoring including electrocardiograms and sometimes holter monitors to detect irregular heartbeats. Treatment depends on arrhythmia type and severity. Some arrhythmias require medication to regulate heart rate. Others require ablation procedures that scar specific heart tissues to prevent irregular electrical signals.
Poor Eye and Muscle Coordination: Vestibulo-Ocular Dysfunction
The vestibulo-ocular reflex coordinates eye movements with head position, allowing you to maintain visual focus while your head moves. This reflex depends on semicircular canals in the inner ear detecting head movement and signaling the eyes to move opposite the head, keeping your visual target centered.
When this reflex deteriorates from aging, neurological disease, or inner ear dysfunction, your eyes cannot keep up with head movements. Vision becomes blurry during head movements, and you experience dizziness trying to maintain balance and visual focus.
Vision also contributes significantly to balance. When vision becomes blurry from cataracts, refractive error, or macular degeneration, balance deteriorates dramatically. Many seniors experience sudden dizziness after cataract surgery when their visual correction suddenly changes.
Treatment involves vision correction through appropriate glasses, cataract surgery when necessary, and vestibular therapy exercises that retrain the vestibulo-ocular reflex. Proprioceptive exercises that strengthen the body’s sense of position in space also help.
Low Blood Sugar: Hypoglycemia and Brain Glucose Deprivation
Hypoglycemia, or abnormally low blood sugar, deprives the brain of its primary fuel source. Blood sugar drops can result from diabetes medication overdosing, skipping meals, excessive exercise, or alcohol consumption without food. As blood sugar drops, the brain becomes glucose-deprived, triggering dizziness, lightheadedness, confusion, and shakiness.
Seniors with diabetes are particularly vulnerable to hypoglycemia because aging reduces the body’s ability to sense low blood sugar and trigger appropriate hunger responses. Medications including insulin and sulfonylureas increase hypoglycemia risk. Many seniors eat infrequently, skipping meals due to loss of appetite, difficulty chewing, or dementia.
Dizziness from hypoglycemia comes on acutely and resolves quickly once blood sugar is restored. Eating simple carbohydrates like juice, candy, or glucose tablets raises blood sugar within minutes.
Prevention requires maintaining regular eating schedules with balanced meals containing protein, fat, and carbohydrates. Diabetes medication adjustments may be necessary as aging affects insulin sensitivity and medication effects. Regular blood sugar monitoring identifies low episodes before they cause severe symptoms.
Creating a Comprehensive Dizziness Evaluation
Rather than accepting dizziness as inevitable, systematic evaluation identifying the specific cause enables targeted treatment. A thorough evaluation includes blood pressure measurements in different positions, complete blood count assessing for anemia, iron studies, metabolic panel assessing electrolytes, thyroid testing, cardiac monitoring, and neurological examination.
Imaging including carotid ultrasound or MRI may be necessary if vascular or neurological causes are suspected. Positional testing helps identify BPPV. Medication review with a pharmacist identifies problematic drug interactions.
Insurance typically covers comprehensive dizziness evaluation, particularly when dizziness causes falls or significantly limits function. Many treatable conditions causing dizziness go undiagnosed simply because patients accept dizziness as normal aging.
Prevention and Management Strategies
Many causes of dizziness are preventable through lifestyle modifications. Maintaining adequate hydration, sufficient salt intake, and regular physical activity prevents orthostatic hypotension and maintains cardiovascular reflexes. Regular vision and hearing assessments catch sensory problems early. Managing blood pressure, cholesterol, and diabetes prevents carotid stenosis progression. Neck strengthening and posture correction prevent cervical spondylosis complications.
Fall prevention becomes critical when managing dizziness in seniors. Environmental modifications including removing tripping hazards, improving lighting, and installing grab bars prevent serious injuries from dizziness-related falls. Balance training exercises strengthen muscles and improve proprioception, reducing fall risk even when dizziness persists.
Medication compliance requires careful attention because missed doses can cause dizziness while overdosing causes dizziness. Pharmacist consultation ensures medications are taken correctly and interactions are identified.
Conclusion: Dizziness is Treatable, Not Inevitable
Orthostatic hypotension from blood pressure drops causes dizziness when standing. Inner ear crystal displacement creates severe vertigo with specific head positions. Carotid artery narrowing reduces brain blood flow. Medication interactions create dangerous drug stacking effects. Anemia and iron deficiency impair oxygen delivery. Neck degeneration compresses vertebral arteries. Dehydration and electrolyte imbalance disrupt balance. Irregular heartbeats interrupt blood flow. Poor eye and muscle coordination disrupt balance reflexes. Low blood sugar deprives the brain of fuel.
Rather than accepting dizziness as inevitable aging, recognize it as a treatable symptom indicating a specific medical problem. Systematic evaluation identifies the underlying cause. Targeted treatment addressing the root problem eliminates dizziness entirely. Your balance system is remarkably responsive to appropriate treatment, restoring your stability, confidence, and quality of life.